
1. Repair
Normal tissue recovers between fractions
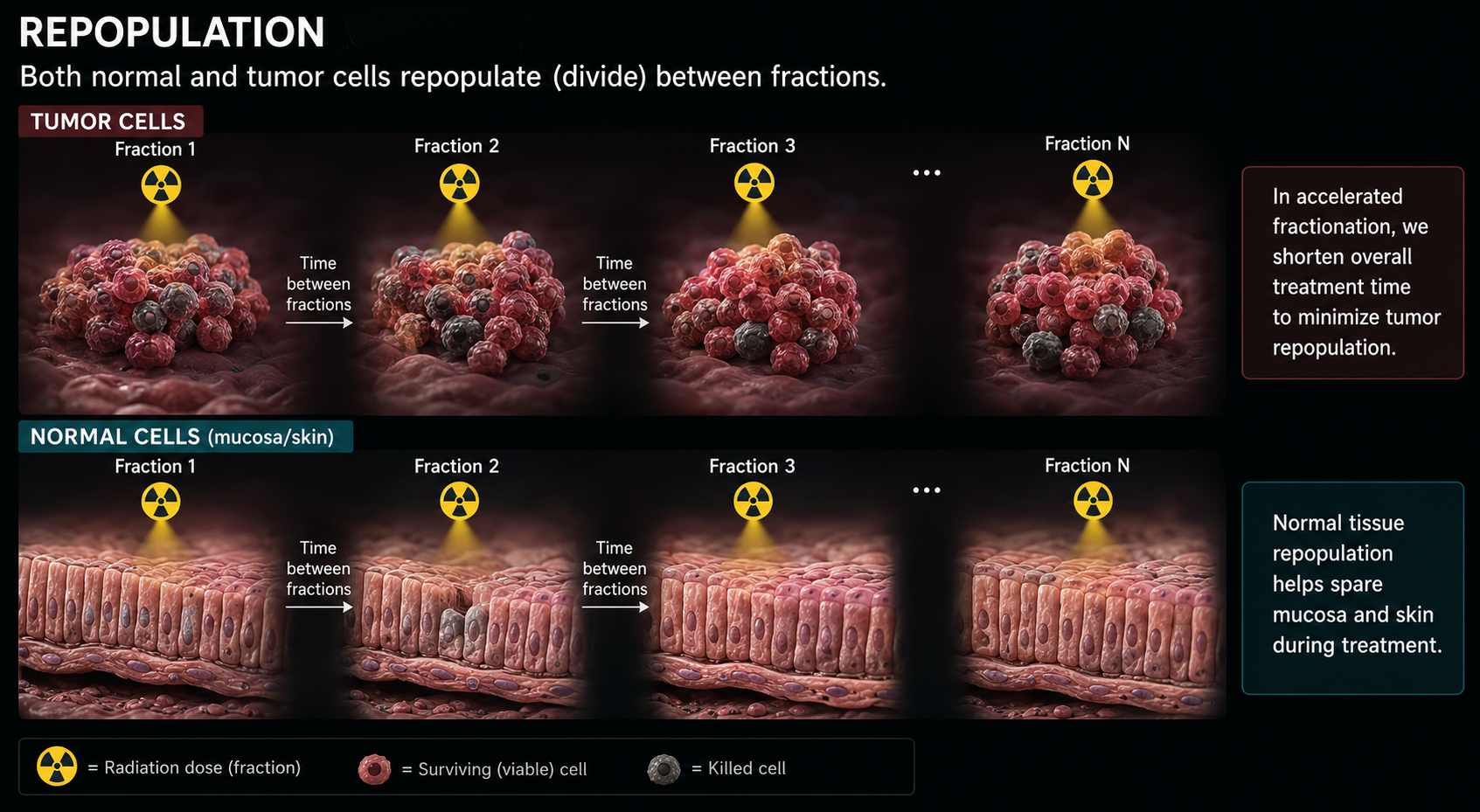
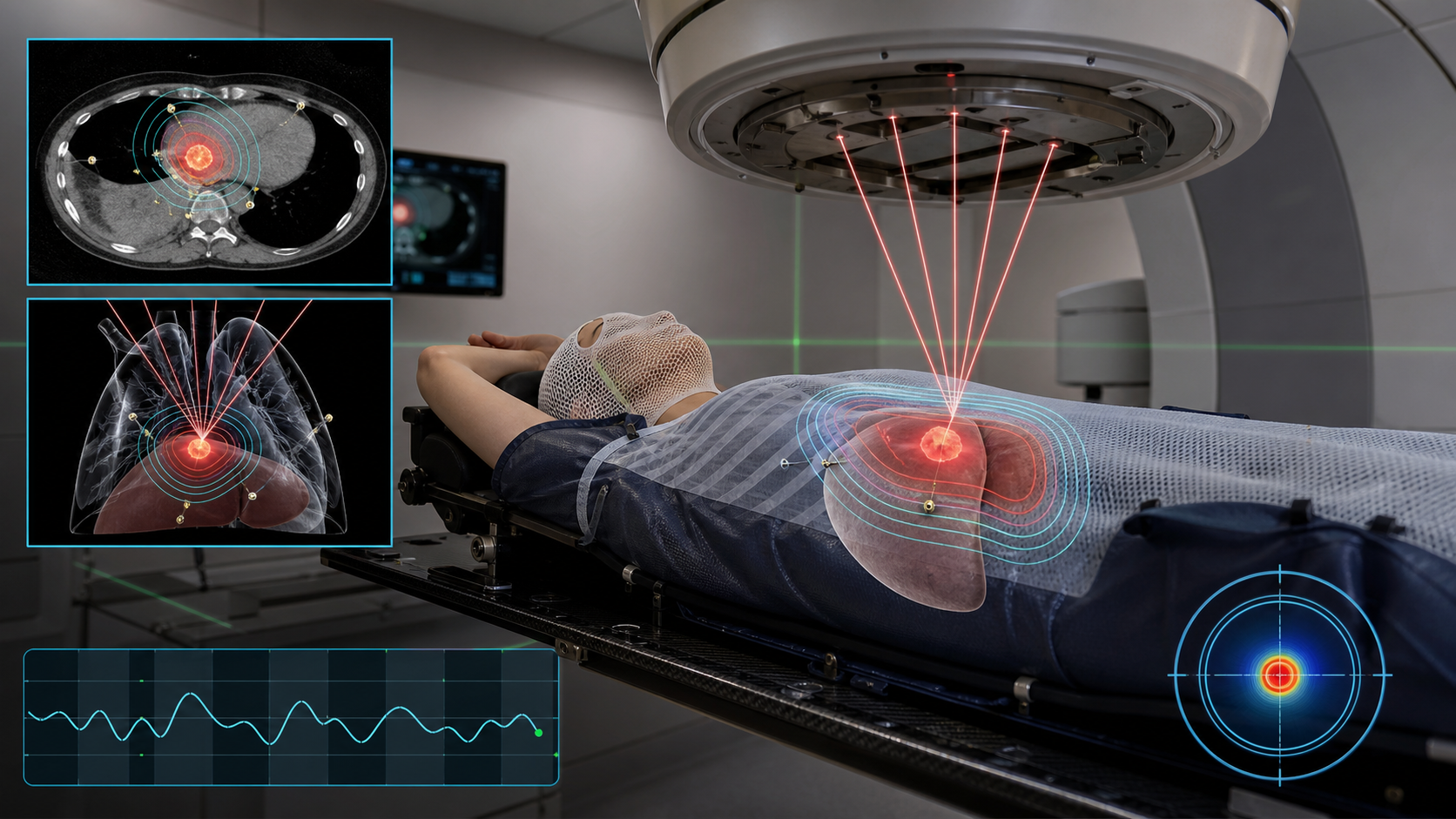
The image shows daily radiation doses injuring both normal and tumor cells, but normal cells repair sublethal DNA damage during the hours to days between fractions. Tumor cells repair less effectively, so damage accumulates across treatments.
Clinical point: fractionation exploits the repair advantage of normal tissue, improving the therapeutic ratio.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}